
Start of text box 1
Overview of the study
This study uses data from the Census of Population and the Longitudinal Immigration Database to paint a picture of immigrants in nursing and health care support occupations. It also examines the representation of immigrants in nursing and health care support occupations by intended occupation upon admission to Canada and by admission category. Lastly, it examines the professional integration of immigrants who completed their nursing education both in and outside Canada.
- Immigrants who arrived in Canada as adults (aged 18 or older) are overrepresented in nursing and health care support occupations. In 2015/2016, they made up 22% of the workforce in these occupations, compared with 16% of the total employed population.
- This overrepresentation of adult immigrants was particularly high for those working in nurse aides, orderlies and patient service associates occupations (30%).
- Overall, 5% of employed adult immigrants in 2015/2016 worked in nursing or health care support occupations, compared with 3% of other employed individuals. However, this proportion varied by place of birth. The percentage of adult immigrants in nursing or health care support occupations was particularly high among immigrants born in the Caribbean and Bermuda (13%), Western Africa (12%), Central Africa (12%), Eastern Africa (8%), and Southeast Asia (10%).
- Among immigrants from Southeast Asia, immigrants from the Philippines stood out with a high proportion (13%) and a large number (44,380) of people employed in nursing or health care support occupations. In 2016, they accounted for nearly one-third (30%) of adult immigrants in these occupations.
- Despite being overrepresented in these occupations, few principal applicants admitted under the economic immigration categories who were working as licensed practical nurses (2%) or nurse aides, orderlies or patient service associates (11%) had considered working in these occupations at the time they were admitted to Canada.
- More than 4 in 10 (44%) adult immigrants in nursing and health care support occupations had completed their highest level of postsecondary education in Canada. However, this proportion varied by place of birth. For example, a large proportion of immigrants from the Caribbean and Bermuda (75%) and sub-Saharan Africa (60%) completed their highest level of education in Canada, while a minority of immigrants born in the Philippines (25%) and Southern Asia (32%) had done so.
- Adult immigrants who graduated outside Canada had significantly higher rates of overqualification than adult immigrants who graduated in Canada. For example, immigrants who completed a bachelor’s degree or higher in a professional nursing program outside Canada were almost four times more likely to be overqualified (58%) than those who completed the same level of education in Canada (15%).
End of text box 1
Introduction
The COVID-19 pandemic has highlighted a number of issues with the workforce in Canada’s health care sector. Labour shortages in some occupations, such as nurses and patient service associates, were exacerbated by the pandemic and received significant media attention. According to data from the Job Vacancy and Wage Survey, most of the increase in the total number of vacancies in Canada in the fourth quarter of 2020 was in health care and social assistance. The number of vacancies in this sector reached an all-time high of 100,300 positions at the end of 2020. However, these challenges have existed for many years and may be exacerbated in the coming decades as the population ages.Note
A number of approaches can be considered to address shortages, such as training more people for these occupations, increasing productivity, reducing absenteeism, raising wages, increasing retention by improving working conditions or attracting more immigrants to fill job vacancies. Turning to the immigrant workforce to fill labour needs for nursing and health care support occupations is common in most countries with advanced health care systems and aging populations.Note As a result, there are major international migration channels involving these workers and to which Canada participates.Note In nursing and health care occupations in Canada, there is significant overrepresentation of people from certain regions of the world, including the Philippines, the Caribbean and sub-Saharan Africa.Note However, little research has explored the driving factors and dynamics behind this overrepresentation.
Some immigrants come to Canada with the specific intention of working in nursing or health care support occupations. In some cases, they come to Canada as a consequence of provincial and territorial policies aimed at recruiting foreign-trained nurses and health care support workers.Note As several studies have shown, however, a range of barriers can hinder the integration of immigrants into the nursing workforce, in particular for registered nurses. These barriers are often related to recognition of foreign qualifications.Note
However, not all immigrants who work in nursing or health care support occupations came to Canada with the intention of working in that field. Many immigrants make a transition to these occupations after arriving in Canada, in part because they experience difficulty finding work.Note These immigrants can help alleviate labour shortages in the same way as those who migrate specifically to work as nurses and health care support workers. Once they complete their studies in Canada, they can often enter the labour market more easily because recognition of their credentials is less of an issue.
There are two main types of pathways immigrants can follow to work in nursing occupations. Each approach can inform public policy in different ways. In the first case, the focus is on admitting immigrants based on pre-arrival training or education, while in the second case the focus is on providing post-arrival training and education to immigrants who were not initially selected specifically to work in nursing and health care support occupations.
This study uses data from the Census of Population and the Longitudinal Immigration Database to paint a picture of immigrants working in nursing and health care support occupations (see the Data sources, methods and definitions box). Particular attention is given to overrepresentation in these occupations by immigrants from certain countries of origin. This study also looks at the representation of immigrants in nursing and health care support occupations in Canada by intended occupation at the time of admission and by admission category. Lastly, this study examines the workforce integration of immigrants who have obtained nursing education in Canada and outside Canada.
For the purposes of this study, the focus will be on immigrants who were 18 or older when they arrived in Canada, as they are the ones who are concerned by issues such as the integration of foreign-educated nurses or career transitions following immigration, not those who arrived at a younger age. They form a group we will refer to as “adult immigrants.”
Immigrants who arrived in Canada as adults are overrepresented in nursing and health care support occupations
In 2015/2016,Note 189,405 immigrants were employed in nursing and health care support occupations, representing 28% of those in these occupations in Canada. In comparison, immigrants represented 24% of the total employed population. However, only immigrants who arrived in Canada as adults were overrepresented in these occupations, while those who arrived at a younger age were slightly underrepresented. Among those working in nursing and health care support occupations, 22% were immigrants who arrived at or after the age of 18 (compared with 16% of the total employed population), and 6% were immigrants who arrived before the age of 18 (7% of the total employed population).
Overall, in Canada, 5% of employed adult immigrants in 2015/2016 worked in nursing or health care support occupations, compared with 3% of other employed individuals. However, this proportion varied by place of birth. In addition, a larger proportion of adult immigrants worked in nursing or health care support occupations in Manitoba (8%), Saskatchewan (7%) and the territories (6%). In contrast, a smaller proportion worked in nursing and health care support occupations in Newfoundland and Labrador (4%), Ontario (4%), and British Columbia (4%).
Start of text box 1
Nursing and health care support occupations
“Nursing and health care support occupations” refers to the following occupational groups from the 2016 National Occupational Classification:
- Professional occupations in nursing comprises the following health care personnel working in the nursing field:
- Nursing co-ordinators and supervisors, who co-ordinate and supervise the activities of registered nurses, registered psychiatric nurses, licensed practical nurses and other nursing personnel in the provision of patient care. This occupation requires completion of a university, college or other approved registered nursing or registered psychiatric nursing program. Courses in management studies or a degree, diploma or certificate in management or administration may also be required.
- Registered nurses and registered psychiatric nurses, who provide nursing care to patients, deliver health care education programs and provide consultative services regarding issues relevant to the practice of nursing. Working in these occupations requires completion of a university degree, college diploma, or completion of another recognized nursing program or a college or university level registered psychiatric nurse program.
- Licensed practical nurses, who provide nursing care to patients, usually under the direction of medical practitioners, registered nurses or other health team members. This occupation requires completion of a vocational, college or other approved program for licensed practical nurses.
- Nurse aides, orderlies and patient service associates, who assist nurses, hospital staff and physicians in the basic care of patients. These occupations require some secondary school and on-the-job training or completion of a nursing aide or health care aide college or private institutional program or a college nursing orderly program and supervised practical training.
End of text box 1
Since the 1990s, the proportion of immigrants in nursing and health care support occupations has grown faster than for other occupations
From 1996 to 2016, the proportion of jobs in nursing and health care support held by adult immigrants in Canada increased overall and in each specific occupational group (Chart 1). The greatest increase was among licensed practical nurses (12 percentage points) and nurse aides, orderlies and patient service associates (12 percentage points).
However, among registered nurses and registered psychiatric nurses and nursing co-ordinators and supervisors, the increase in the proportion of adult immigrants reflects the trend observed in the total employed population. Adult immigrants are even underrepresented among nursing co-ordinators and supervisors.

Data table for Chart 1
| Occupational group | 1996 | 2006 | 2016 |
|---|---|---|---|
| percentage | |||
| All nursing and health care support occupations | 13.7 | 16.2 | 21.9 |
| Nursing co-ordinators and supervisors | 9.5 | 10.3 | 11.4 |
| Registered nurses and registered psychiatric nurses | 12.8 | 14.0 | 15.9 |
| Licensed practical nurses | 9.0 | 12.3 | 21.2 |
| Nurse aides, orderlies and patient service associates | 17.2 | 20.9 | 29.5 |
| Other occupations | 12.7 | 14.4 | 16.1 |
Immigrants born in the Caribbean and Bermuda, sub-Saharan Africa, and the Philippines were most likely to work in nursing or health care support occupations
The proportion of immigrants in nursing or health care support occupations varied significantly by region or country of birth. It was particularly high for adult immigrants born in the Caribbean and Bermuda (13%), Western Africa (12%), Central Africa (12%), Eastern Africa (8%), and Southeast Asia (10%) (Table 1), compared with all adult immigrants in these occupations (5%). In addition, a significant number of workers in nursing and health care support occupations were born in other regions or countries that were not overrepresented in these occupations: India (12,225 workers, or 3%), China (5,515, or 2%), the United Kingdom (3,555, or 3%) and Poland (2,965, or 5%).
Among adult immigrants from Southeast Asia, those from the Philippines stood out with a high proportion (13%) and a large number (44,380) of workers in nursing and health care support occupations. They accounted for nearly one-third (30%) of adult immigrants in these occupations.
Although adult immigrants born in the majority of countries in the Caribbean and Bermuda and sub-Saharan AfricaNote are overrepresented in nursing and health care support occupations, there was some variation among countries in the same region. For example, 25% of Haitian-born adult immigrants were in nursing and health care support occupations, nearly double the proportion for those born in Jamaica (13%).
Adult immigrants born in the Caribbean and Bermuda, in Western, Central or Eastern Africa, and in the Philippines were overrepresented in each of the specific nursing and health care support occupational groups. However, the representation of immigrants born in these regions was particularly high among nurse aides, orderlies and patient service associates. Among adult immigrants from these regions who worked in nursing and health care support occupations, 57% to 64% worked as nurse aides, orderlies or patient service associates, compared with 36% for other workers (see the Distribution of workers in nursing and health care support occupations, by occupation and region or country of birth – 2015/2016 box).
| Region of birth/country of birth (selected cases) | Total number of employed persons | Total number of persons employed in nursing and health care support occupations | Total number of employed women | Total number of women employed in nursing and health care support occupations | Proportion of all employed persons in nursing and health care support occupations | Proportion of all employed men in nursing and health care support occupations | Proportion of all employed women in nursing and health care support occupations |
|---|---|---|---|---|---|---|---|
| number | percentage | ||||||
| All workers | 19,956,255 | 676,155 | 9,613,280 | 606,565 | 3.4 | 0.7 | 6.3 |
| All adult immigrant workers | 3,243,670 | 147,705 | 1,567,400 | 128,010 | 4.5 | 1.2 | 8.2 |
| All other workersTable 1 Note 1 | 16,712,585 | 528,445 | 8,045,880 | 478,555 | 3.2 | 0.6 | 6.0 |
| United States | 81,955 | 2,245 | 44,390 | 1,975 | 2.7 | 0.7 | 4.5 |
| Central America | 80,240 | 2,395 | 36,945 | 2,060 | 3.0 | 0.8 | 5.6 |
| Caribbean and Bermuda | 167,360 | 22,220 | 89,490 | 20,270 | 13.3 | 2.5 | 22.6 |
| Haiti | 44,470 | 10,880 | 24,055 | 9,575 | 24.5 | 6.4 | 39.8 |
| Jamaica | 55,085 | 7,250 | 29,785 | 6,935 | 13.2 | 1.2 | 23.3 |
| South America | 153,730 | 5,100 | 78,275 | 4,585 | 3.3 | 0.7 | 5.9 |
| Guyana | 37,360 | 1,680 | 19,230 | 1,585 | 4.5 | 0.5 | 8.2 |
| Western Europe | 116,520 | 2,655 | 52,405 | 2,340 | 2.3 | 0.5 | 4.5 |
| Eastern Europe | 252,155 | 9,315 | 129,150 | 8,495 | 3.7 | 0.7 | 6.6 |
| Poland | 64,395 | 2,965 | 33,025 | 2,805 | 4.6 | 0.5 | 8.5 |
| Romania | 52,850 | 1,895 | 26,330 | 1,720 | 3.6 | 0.7 | 6.5 |
| Northern Europe | 140,630 | 4,085 | 61,480 | 3,675 | 2.9 | 0.5 | 6.0 |
| United Kingdom | 121,385 | 3,555 | 52,925 | 3,185 | 2.9 | 0.5 | 6.0 |
| Southern Europe | 130,890 | 2,225 | 54,015 | 2,015 | 1.7 | 0.3 | 3.7 |
| Western Africa | 63,605 | 7,360 | 28,170 | 5,965 | 11.6 | 3.9 | 21.2 |
| Nigeria | 24,475 | 3,425 | 11,145 | 2,780 | 14.0 | 4.8 | 25.0 |
| Ghana | 12,945 | 1,670 | 5,950 | 1,460 | 12.9 | 3.0 | 24.6 |
| Eastern Africa | 95,235 | 7,750 | 44,105 | 6,525 | 8.1 | 2.4 | 14.8 |
| Ethiopia | 20,230 | 2,300 | 9,090 | 1,930 | 11.4 | 3.3 | 21.3 |
| Northern Africa | 118,990 | 3,600 | 46,325 | 2,185 | 3.0 | 1.9 | 4.7 |
| Morocco | 38,630 | 1,705 | 15,350 | 1,140 | 4.4 | 2.4 | 7.4 |
| Central Africa | 27,980 | 3,320 | 13,010 | 2,705 | 11.9 | 4.1 | 20.8 |
| Democratic Republic of the Congo | 12,440 | 1,695 | 5,825 | 1,380 | 13.6 | 4.8 | 23.7 |
| Cameroon | 11,180 | 1,330 | 5,380 | 1,085 | 11.9 | 4.3 | 20.1 |
| Southern Africa | 21,340 | 505 | 9,870 | 455 | 2.4 | 0.5 | 4.6 |
| West Central Asia and the Middle East | 235,385 | 3,395 | 94,395 | 2,805 | 1.4 | 0.4 | 3.0 |
| Eastern Asia | 481,320 | 9,015 | 251,745 | 8,005 | 1.9 | 0.4 | 3.2 |
| China | 313,560 | 5,515 | 161,995 | 4,905 | 1.8 | 0.4 | 3.0 |
| Southeast Asia | 478,420 | 45,940 | 277,410 | 39,555 | 9.6 | 3.2 | 14.3 |
| Philippines | 354,410 | 44,380 | 212,325 | 38,190 | 12.5 | 4.4 | 18.0 |
| Southern Asia | 570,520 | 15,190 | 244,180 | 13,150 | 2.7 | 0.6 | 5.4 |
| India | 377,560 | 12,225 | 169,120 | 10,665 | 3.2 | 0.8 | 6.3 |
| Oceania | 27,130 | 1,375 | 11,900 | 1,225 | 5.1 | 1.0 | 10.3 |
The vast majority of workers in nursing and health care support occupations are women
Nursing and health care support jobs are largely held by women. In 2016, nearly 9 in 10 workers in these occupations were women. Overall, the proportion of female adult immigrants (87%) and male adult immigrants (13%) in nursing and health care support occupations was similar to the proportion for non-immigrants and immigrants who arrived in Canada before age 18 (91% for women and 9% for men). However, variations by region or country of birth were observed. For example, there was a high proportion of males among African-born immigrants—close to 20% among immigrants born in Western, Central and Eastern Africa and close to 40% among those born in Northern Africa.
Adult immigrant women born in the Caribbean and Bermuda (23%), sub-Saharan Africa (16%) or the Philippines (18%) were more likely to work in nursing or health care support occupations compared with other immigrant women. Overall, about one in five women from these regions worked in one of these occupations in 2016, compared with just over one in 20 (6%) for non-immigrant women or immigrant women who arrived in Canada before age 18.
Among the countries of origin, adult immigrant women born in Haiti (40%), Nigeria (25%) or Ghana (25%) were among the most likely to work in nursing or health care support occupations.
The increase in the proportion of immigrants working in nursing and health care support occupations is due largely to immigrants from the Philippines and sub-Saharan Africa
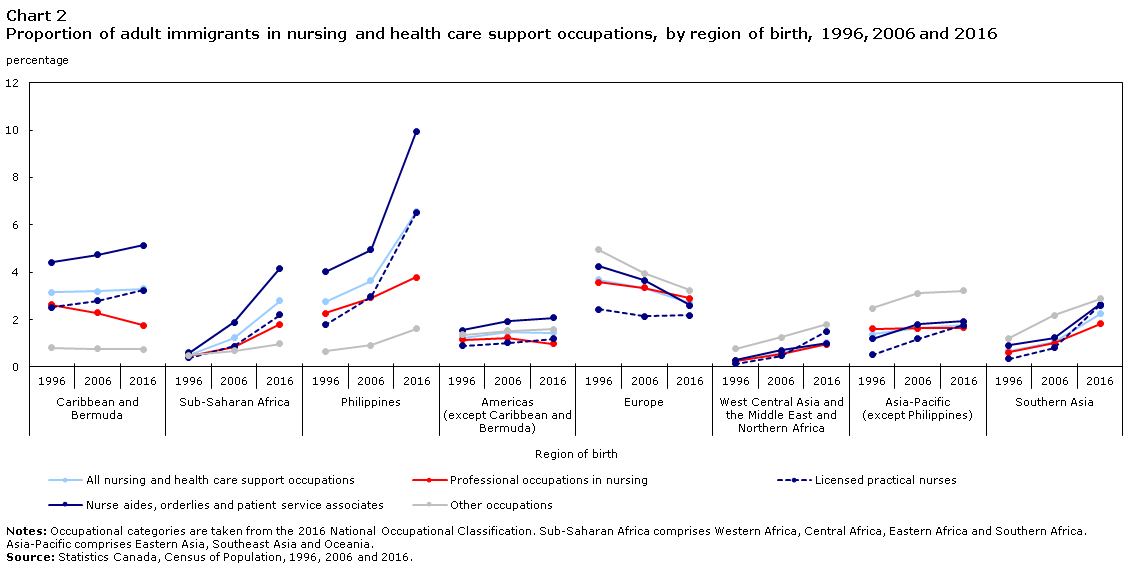
Changes over time in the proportion of immigrants in nursing and health care support occupations vary by place of birth (Chart 2). Thus, we can see that the increase in the proportion of adult immigrants in nursing and health care support occupations from 1996 to 2016 was due mainly to the large increase in the number of workers from the Philippines and sub-Saharan Africa.
The proportion of workers from the Caribbean and Bermuda in these occupations was relatively stable from 1996 to 2016 (about 3%), while there was a marked increase in the proportion of immigrants from sub-Saharan Africa (increased from 0.5% to 3%) and the Philippines (increased from 3% to 7%).
During this period, the proportion of immigrants born in the Philippines working as nurse aides, orderlies and patient service associates grew particularly rapidly. In 2016, about 10% of all nurse aides, orderlies and patient service associates in Canada were adult immigrants from the Philippines, compared with 4% in 1996.
Data table for Chart 2
| Occupational group | Caribbean and Bermuda |
Sub-Saharan Africa | Philippines | Americas (except Caribbean and Bermuda) |
Europe | West Central Asia and the Middle East and Northern Africa | Asia-Pacific (except Philippines) |
Southern Asia | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1996 | 2006 | 2016 | 1996 | 2006 | 2016 | 1996 | 2006 | 2016 | 1996 | 2006 | 2016 | 1996 | 2006 | 2016 | 1996 | 2006 | 2016 | 1996 | 2006 | 2016 | 1996 | 2006 | 2016 | |
| percentage | ||||||||||||||||||||||||
| All nursing and health care support occupations | 3.2 | 3.2 | 3.3 | 0.5 | 1.2 | 2.8 | 2.8 | 3.6 | 6.6 | 1.2 | 1.5 | 1.4 | 3.7 | 3.4 | 2.7 | 0.3 | 0.6 | 1.0 | 1.4 | 1.7 | 1.8 | 0.7 | 1.1 | 2.3 |
| Professional occupations in nursing | 2.6 | 2.3 | 1.8 | 0.5 | 0.9 | 1.8 | 2.3 | 2.9 | 3.8 | 1.2 | 1.2 | 1.0 | 3.6 | 3.4 | 2.9 | 0.3 | 0.6 | 1.0 | 1.6 | 1.6 | 1.7 | 0.6 | 1.0 | 1.8 |
| Licensed practical nurses | 2.5 | 2.8 | 3.2 | 0.4 | 0.9 | 2.2 | 1.8 | 3.0 | 6.5 | 0.9 | 1.0 | 1.2 | 2.4 | 2.2 | 2.2 | 0.1 | 0.5 | 1.5 | 0.5 | 1.2 | 1.8 | 0.3 | 0.8 | 2.6 |
| Nurse aides, orderlies and patient service associates | 4.4 | 4.7 | 5.1 | 0.6 | 1.9 | 4.2 | 4.0 | 5.0 | 9.9 | 1.5 | 1.9 | 2.1 | 4.3 | 3.7 | 2.6 | 0.3 | 0.7 | 1.0 | 1.2 | 1.8 | 1.9 | 0.9 | 1.2 | 2.7 |
| Other occupations | 0.8 | 0.8 | 0.8 | 0.5 | 0.7 | 1.0 | 0.7 | 0.9 | 1.6 | 1.4 | 1.5 | 1.6 | 5.0 | 4.0 | 3.2 | 0.8 | 1.3 | 1.8 | 2.5 | 3.1 | 3.2 | 1.2 | 2.2 | 2.9 |
The proportion of immigrants admitted under the economic immigrant categories who planned to work in nursing and health care support occupations has been particularly high since 2010
There are two main pathways adult immigrants can take to work in nursing and health care support occupations: (1) training in the field abroad and coming to Canada to work in one of these occupations and (2) training for and transitioning to these occupations after arrival. These pathways are explored in the following sections using data from the Longitudinal Immigration Database, which provides information on the intended occupation of economic immigrant principal applicants at the time of their admission to Canada as permanent residents.
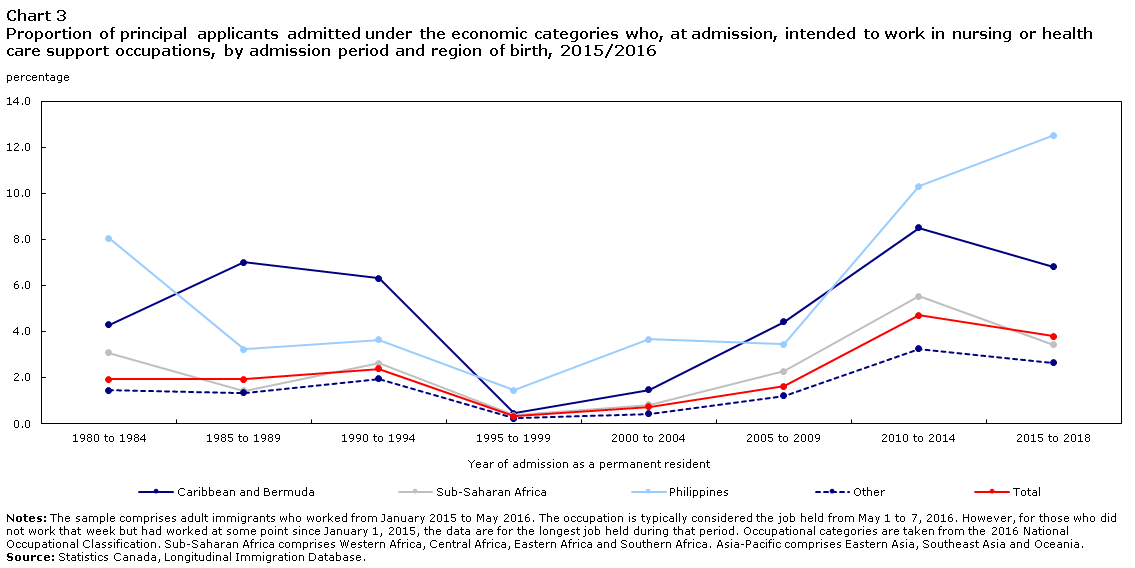
Since 1980, the proportion of immigrants admitted under the economic immigrant categories (principal applicants only) intending to work in nursing or health care support occupations has fluctuated by year of admission as a permanent resident, i.e., landing year (Chart 3). Among immigrants who landed between 1980 and 1994, this proportion remained relatively stable, at about 2%. The proportion then dropped to a low for the 1995 to 1999 landing cohorts but gradually increased beginning in 2000 and has remained at about 4% since 2010.Note
Proportionally, for immigrants admitted under the economic immigrant categories, the trend for intended occupation was generally the same for all regions or countries of birth. However, immigrants from the Philippines, the Caribbean and Bermuda, and sub-Saharan Africa were significantly more likely to declare one of the nursing and health care support occupations as their intended occupation upon admission to Canada than those from elsewhere, reflecting their overrepresentation in these occupations. Similar to what was observed among immigrants from other regions, the number of immigrants from these regions who intended to work in one of these occupations began increasing in 2000, following a low in the 1995–1999 admission cohort. From 2015 to 2018, the proportion of immigrants admitted under the economic immigrant categories from these three regions who had such intentions were 13%, 7% and 3%, respectively.
Data table for Chart 3
| Admission period | Total | Region of birth | |||
|---|---|---|---|---|---|
| Caribbean and Bermuda | Sub-Saharan Africa | Philippines | Other | ||
| percentage | |||||
| 1980 to 1984 | 1.9 | 4.3 | 3.1 | 8.1 | 1.5 |
| 1985 to 1989 | 1.9 | 7.0 | 1.4 | 3.2 | 1.3 |
| 1990 to 1994 | 2.4 | 6.3 | 2.6 | 3.7 | 1.9 |
| 1995 to 1999 | 0.3 | 0.4 | 0.4 | 1.5 | 0.2 |
| 2000 to 2004 | 0.7 | 1.5 | 0.8 | 3.7 | 0.4 |
| 2005 to 2009 | 1.6 | 4.4 | 2.3 | 3.4 | 1.2 |
| 2010 to 2014 | 4.7 | 8.5 | 5.5 | 10.3 | 3.3 |
| 2015 to 2018 | 3.8 | 6.8 | 3.4 | 12.5 | 2.6 |
Few immigrants working as nurse aides, orderlies or patient service associates intended to work in these occupations upon admission
Knowledge of whether immigrants admitted under the economic categories are actually working in the occupations they intended to work in at the time of admission is important for immigration admission and integration policy-making. If immigrants are not working in their intended occupation, the question arises as to whether they are working in another health care occupation and, if so, whether the occupation is consistent with their qualifications. For example, professional occupations in nursing require a higher level of skill than for licensed practical nurse occupations, which in turn require a higher level of skill for than the occupations of nurse aide, orderly and patient service associates.
Of the economic immigrant principal applicants who intended upon admission to work in a professional occupation in nursing to Canada, nearly half (48%) were in fact working in an occupation in this group in 2015/2016 (Table 2).Note In contrast, 23% were working in another nursing or health care support occupation, but a sizeable proportion (29%) were working in other types of occupations, often in low-skilled jobs.
About one-quarter of those who intended to work as a licensed practical nurse (22%) or as a nurse aide, orderly or patient service associate (26%) were actually working in one of these occupations in 2015/2016.
Of the immigrant women who intended to work as a licensed practical nurse, 22% were actually working in that occupation; however, 39% were working in professional occupations in nursing. This finding suggests that many of these immigrant women who wanted to work as licensed practical nurses had pursued additional postsecondary education after their admission as permanent residents to advance their careers.
A similar scenario was observed, albeit to a lesser extent, for immigrant men who intended to work as a nurse aide, orderly or patient service associate. While 26% worked in one of these occupations in 2015/2016, 19% were working as a licensed practical nurse or in one of the professional occupations in nursing.
| Occupation held in 2015 and 2016 | Intended occupation at time of admission | ||
|---|---|---|---|
| Professional occupations in nursing | Licensed practical nurses | Nurse aides, orderlies and patient service associates | |
| percentage | |||
| Professional occupations in nursing | 48 | 39 | 13 |
| Licensed practical nurses | 6 | 22 | 6 |
| Nurse aides, orderlies and patient service associates | 14 | 12 | 26 |
| Other health occupations | 3 | 3 | 4 |
| Non-health occupations, usually requiring a postsecondary diploma | 12 | 11 | 15 |
| Non-health occupations, usually requiring a high school diploma or less | 17 | 13 | 35 |
| Total | 100 | 100 | 100 |
For all economic immigrant principal applicants who were working as a nurse aide, orderly or patient service associate in 2015/2016, 2% had intended to work in that occupation upon admission to Canada (Table 3). Although the proportion was slightly higher for those working as a licensed practical nurse (11%), it was still low. Thus, despite the fact that adult immigrants are particularly overrepresented in these occupations, the vast majority of economic immigrant principal applicants holding these jobs did not, upon admission to Canada, intend to work in these occupations. These results show that immigrants from all backgrounds can help address the shortage of workers in these occupations, not just those who originally intend to work in the health care field.
The picture was somewhat different among professional occupations in nursing, where 50% of economic immigrant principal applicants working in this occupation originally intended to do so. Together, these results illustrate that it can be difficult to predict, on the basis of intended occupations declared at admission, the actual number of immigrants entering under the economic immigrant categories who will actually work in nursing or health care support occupations.
| Intended occupation at time of admission | Occupation held in 2015 and 2016 | ||
|---|---|---|---|
| Professional occupations in nursing | Licensed practical nurses | Nurse aides, orderlies and patient service associates | |
| percentage | |||
| Professional occupations in nursing | 50 | 22 | 13 |
| Licensed practical nurses | 6 | 11 | 1 |
| Nurse aides, orderlies and patient service associates | 1 | 2 | 2 |
| Other health occupations | 5 | 6 | 6 |
| Non-health occupations, usually requiring a postsecondary diploma | 18 | 30 | 22 |
| Non-health occupations, usually requiring a high school diploma or less | 19 | 29 | 56 |
| Total | 100 | 100 | 100 |
Working in a nursing or health care support occupation is largely independent of the category of admission to Canada
Although the majority of those who migrated to Canada with the intention to work in nursing or health care support occupations are principal and secondary applicants admitted under the economic immigrant categories, immigrants admitted under other categories also end up working in these occupations.
Table 4 presents the proportion of adult immigrant applicants admitted under different admission categories who were employed in nursing and health care support occupations in 2015/2016. Compared with those admitted under the other admission categories, principal applicants admitted under the economic immigrants category were slightly more likely to be employed in nursing or health care support occupations (5.1%). Overall, however, employment in nursing and health care support occupations was not specific to any particular immigration category.
| Admission category | Occupation held | |||
|---|---|---|---|---|
| Professional occupations in nursing | Licensed practical nurses | Nurse aides, orderlies and patient service associates | Total (nursing and health care support occupations) | |
| percentage | ||||
| Immigrants admitted under economic categories – Principal applicants | 1.9 | 0.6 | 2.7 | 5.1 |
| Immigrants admitted under economic categories – Secondary applicants | 1.6 | 0.6 | 2.2 | 4.4 |
| Immigrants sponsored by family | 1.4 | 0.5 | 2.5 | 4.4 |
| Refugees | 1.2 | 0.4 | 2.9 | 4.6 |
| Total (all categories) | 1.6 | 0.5 | 2.6 | 4.6 |
A major exception is observed, however, for immigration programs aimed specifically at caregivers, who fall under the economic immigrant categories. Of the principal applicants admitted under these programs, 20% worked in nursing or health care support occupations, with 4% working as professional nurses, 2% as licensed practical nurses and 15% as nurse aides, orderlies or patient service associates. Immigrants from the Philippines accounted for 87% of adult immigrants admitted under these programs and who were employed in 2015/2016. Among adult immigrants from the Philippines who worked in nursing or health care support occupations, 48% had been admitted to Canada under one of the caregivers programs (compared with less than 3% of other adult immigrants in these occupations).Note The overrepresentation of Filipino immigrants in nursing occupations can, therefore, be explained in part by the very high number of this group of immigrants admitted to Canada under these programs.
In general, however, the relationship between immigration category and working in these occupations is relatively weak. Immigrants admitted under all major immigration categories—economic, family-sponsored and refugee—enter these occupations in relatively similar proportions. For example, immigrants in the family-sponsored and refugee categories respectively accounted for 30% and 13% of adult immigrants working in nursing and health care support occupations in 2015/2016 (compared with 32% and 13%, respectively, among all other occupations). These categories accounted for the majority of immigrants from the Caribbean and Bermuda (62%) and sub-Saharan Africa (65%) working in nursing and health care support occupations.
In summary, considering the weak relationship between the intended occupation and the actual occupation of economic immigrant principal applicants, as well as the similar representation of immigrants admitted under different admission categories, we are led to think that a large portion of adult immigrants working in nursing and health care support occupations only moved into these occupations after moving to Canada.
A majority of workers from the Caribbean and Bermuda and sub-Saharan Africa completed their highest level of postsecondary education in Canada
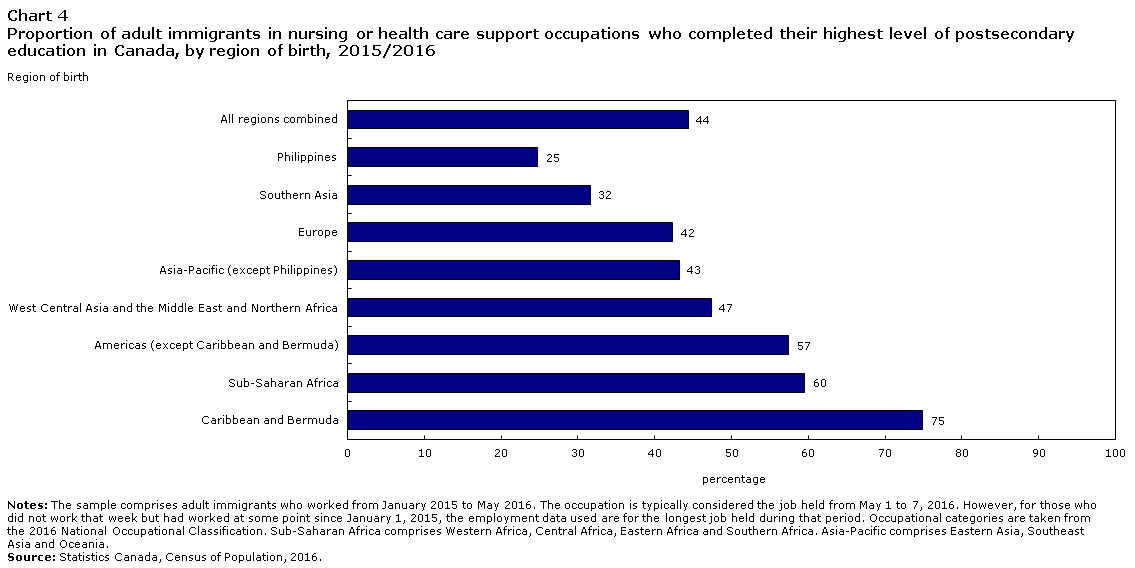
Immigrants admitted under all admission categories who transitioned to other occupations may have done so by completing education in Canada. A total of 44% of adult immigrants in nursing and health care support occupations in 2015/2016 completed their highest level of postsecondary education in Canada. This proportion was 44% among those working in professional nursing occupations, 51% among those working as licensed practical nurses, and 43% among nurse aides, orderlies and patient service associates. In comparison, among immigrants working in other occupations requiring a postsecondary degree or diploma, 27% earned their highest postsecondary degree or diploma in Canada.
The proportion of adult immigrants who completed their highest level of postsecondary education in Canada varied by region of birth (Chart 4). Among those working in all nursing and health care support occupations, the majority of immigrants from the Caribbean and Bermuda (75%) and sub-Saharan Africa (60%) completed their highest level of postsecondary education in Canada. In contrast, a minority of immigrants born in the Philippines (25%) and Southern Asia (32%) were graduates of a program in Canada. For the remaining immigrants, the breakdown was more consistent between those who were graduates of a program in Canada and those of a program outside Canada.Note
Data table for Chart 4
| Region of birth | Proportion of adult immigrants who completed their highest level of education in Canada |
|---|---|
| percentage | |
| Caribbean and Bermuda | 75 |
| Sub-Saharan Africa | 60 |
| Americas (except Caribbean and Bermuda) | 57 |
| West Central Asia and the Middle East and Northern Africa | 47 |
| Asia-Pacific (except Philippines) | 43 |
| Europe | 42 |
| Southern Asia | 32 |
| Philippines | 25 |
| All regions combined | 44 |
The field of study in which workers attained their highest level of education is not necessarily directly related to the job they hold. For example, among adult immigrants working in nursing and health care support occupations who completed their education outside Canada, 55% had studied in a field related to these occupations, compared with 84% of those who graduated in Canada.
There are several possible explanations for immigrants completing training for nursing and health care support occupations in Canada after migration.Note Immigrants may, for one reason or another, decide to make a transition to a nursing or health care support occupation in Canada following their arrival. Younger people in particular may be completing education they began in their country of origin. Individuals who studied in a nursing or health care support program or worked in such an occupation prior to their immigration may have decided to return to school to advance their career. Lastly, immigrants may have completed their nursing program outside Canada but, because of barriers to having their foreign qualifications recognized, they return to school to increase their chances of finding a job.Note These different trajectories have all been documented in Canada.Note However, because data on the initial field of study of those who continue their studies in Canada are not available, it is difficult to differentiate them and to determine their respective scope.
High level of overqualification among immigrant workers who completed their education outside Canada
Many studies have found that immigrants who completed their postsecondary education in Canada are less likely to be overqualified. The same could also be true for nursing and health care support occupations. The table in the Occupation held by adult immigrants, by field and location of study – 2015/2016 box presents the occupations held by adult immigrant graduates of different types of educational programs, by location of study. Overall, it shows that immigrants who graduated from nursing programs outside Canada were significantly less likely to enter occupations matching their educational background than those who graduated from programs in Canada. For example, 37% of immigrants who completed a bachelor’s degree or higher in a professional nursing program outside Canada were employed in these occupations, compared with 78% of those who completed their education in Canada.
For those with a postsecondary degree, this information was captured using an “overqualification rate,” which corresponds to the proportion of graduates employed in an occupation requiring a lower level of education than what they possess. Table 5 presents the overqualification rates calculated for adult immigrant graduates of different types of programs, by location of study and region of birth. The rates were adjusted for age and province of residence.
| Region of birth | Overqualification rate by major field of study | ||
|---|---|---|---|
| Licensed practical nurses | Registered nurses, nursing administration, nursing research and clinical nursing | ||
| Diploma below bachelor level | Bachelor’s degree or higher | ||
| percentage | |||
| Non-immigrants and immigrants who were under the age of 18 at time of admission | 23 | 20 | 11 |
| Adult immigrants – Studies in Canada | 24 | 33 | 15 |
| Caribbean and Bermuda | 24 | 32 | 14 |
| Sub-Saharan Africa | 29 | 39 | 17 |
| Philippines | 24 | 38 | 24 |
| Americas (except Caribbean) | 30 | 34 | 10 |
| Europe | 18 | 23 | 9 |
| West Central Asia and the Middle East and Northern Africa | 20 | 43 | 16 |
| Asia-Pacific (except Philippines) | 21 | 38 | 8 |
| Southern Asia | 25 | 31 | 23 |
| Adult immigrants – Studies outside Canada | 55 | 44 | 58 |
| Caribbean and Bermuda | 56 | 44 | 37 |
| Sub-Saharan Africa | 56 | 44 | 42 |
| Philippines | 65 | 56 | 67 |
| Americas (except Caribbean) | 57 | 41 | 39 |
| Europe | 46 | 36 | 30 |
| West Central Asia and the Middle East and Northern Africa | 44 | 54 | 49 |
| Asia-Pacific (except Philippines) | 58 | 37 | 47 |
| Southern Asia | 62 | 45 | 48 |
In general, adult immigrants who graduated outside Canada had significantly higher rates of overqualification than those who graduated in Canada. The highest rates of overqualification were typically observed among those who had completed a bachelor’s degree or higher from a professional nursing program outside Canada (58%) and those who had completed a program qualifying them to work as a licensed practical nurse (55%).
However, these rates varied by region of birth. For example, foreign graduates from the Philippines had high rates of overqualification, up to 67% among those with a bachelor’s degree or higher from a professional nursing program. This is consistent with findings of other studies showing a clear trend towards overqualification in Canada among graduates from the Philippines.Note
Although they were less likely to be overqualified than those that held a foreign degree, adult immigrants with a Canadian bachelor’s degree or higher from a professional nursing program generally had higher rates of overqualification (15%) than non-immigrants and immigrants who arrived in Canada before the age of 18 (11%). Adult immigrants from the Philippines were again found to have the highest rates of overqualification among those with a bachelor’s degree or higher obtained in Canada (24%). The rate of overqualification for adult immigrants who studied in a licensed practical nursing program in Canada (24%) was similar to that of non-immigrants and immigrants who arrived in Canada before age 18 (23%).
What accounts for the differences by origin among those who studied in Canada? First, adult immigrants may experience more difficulties than non-immigrants, even if they completed only part of their education outside Canada. Indeed, because location of education is determined by the location where the highest level of education was completed, in some cases individuals will also have done part of their studies outside Canada, which may be a differentiating factor. Second, aside from education, recognition of foreign work experience may be a factor for adult immigrants. Last, the differences could also be explained by broader challenges accessing skilled employment, such as lower proficiency in Canada’s official languages or discrimination, or by individual migration and career strategies making some people more willing, for one reason or another, to accept a job for which they are overqualified.
Conclusion
Immigrants who arrived in Canada as adults are overrepresented in nursing and health care support occupations, particularly among nurse aides, orderlies and patient service associates and licensed practical nurses. This is due in large part to the high overrepresentation of immigrants from the Caribbean and Bermuda, sub-Saharan Africa, and the Philippines in all these occupations. In particular, the representation of immigrants from sub-Saharan Africa and the Philippines in these occupations has noticeably increased from 1996 to 2016, whereas immigrants from other regions were often underrepresented in these occupations.
Immigrants from the Philippines accounted for nearly one-third of adult immigrants in nursing and health care support occupations. The majority are immigrants admitted under the economic immigrant categories, most of whom were the principal applicants. In fact, half were admitted under programs offering a pathway to permanent residence for caregivers. Three-quarters of immigrants from the Philippines whose highest level of education was in nursing had completed their education abroad. Obtaining employment in a nursing occupation was difficult for them, and two thirds were overqualified.
For several decades, immigrants from the Caribbean have been overrepresented in nursing and health care support occupations, while the overrepresentation of immigrants from sub-Saharan Africa has increased over the past 20 years. In both cases, only a minority of those working in nursing and health care support occupations were immigrants admitted under the economic immigrants category and a majority had completed their highest level of education in Canada. Their overrepresentation in these occupations is due to the fact that they were particularly likely to transition to these occupations after arriving in Canada.
Among principal applicants under the economic immigrant categories who had intended to work in nursing or health care support occupations when they were admitted, the vast majority intended to work as registered nurses or registered psychiatric nurses, and half of those working as registered nurses or registered psychiatric nurses in 2015/2016 had intended to do so when they were admitted. Conversely, the vast majority of immigrants admitted under the economic immigrant categories who were working as licensed practical nurses, nurse aides, orderlies and patient service associates had not intended to work in these occupations at the time of their admission.
A large share of immigrants in nursing and health care support occupations were not admitted under the economic immigrant categories. In fact, admission category appeared to have relatively little bearing on whether the person worked in these occupations, compared with country of birth. In addition, although it varied by region or country of birth and immigration category, a significant share of adult immigrants working in these occupations completed their highest level of education in Canada.
These findings show that a significant proportion of adult immigrants working in nursing and health care support occupations transitioned into these occupations after arriving in Canada—a transition that often involved going back to school. This raises important considerations for policies that focus on immigration as a solution to labour shortages in nursing and health care support occupations, since it shows that post-arrival reorientation and retraining into these occupations is the key moment behind many immigrants’ contribution to the field.
On the other hand, relying on foreign-trained workers appears to be hindered by difficulties related to credentials recognition and access to professional nursing occupations. Approximately half of graduates of foreign programs that qualified them for professional occupations in nursing or as licensed practical nurses were overqualified for the job they held in Canada.
These findings also raise questions about what motivates some immigrants to choose nursing and health care support occupations after their arrival in Canada. They also highlight the importance of exploring the complex relationship between immigration and the labour market, one that varies greatly by gender and place of origin.
This study is based on data from the 2016 Census and thus the situation may have changed somewhat since then. For example, it has been found that a high number of people arriving in Montréal seeking refugee protection in recent years went on to work as orderlies.Note In addition, the COVID-19 pandemic has had a significant effect on the health care workforce. This study does not take into account these recent developments.
Louis Cornelissen is an analyst with the Diversity and Sociocultural Statistics Division.
Start of text box 2
Data sources, methods and definitions
Data sources
The data used in this article are from the 1996, 2006 and 2016 censuses, as well as from the Longitudinal Immigration Database.
Intended occupation
Information on the intended occupation of immigrants upon their admission to Canada is from the Longitudinal Immigration Database (IMDB). In order to compare the intended occupation at the time of admission with the occupation held in 2015/2016, a linkage between the IMDB data and the 2016 Census data was used.
As part of the process for becoming a permanent resident, principal applicants under the economic immigrant categories are required to report their intended occupation in Canada. To declare an intended occupation, applicants must demonstrate that they have the educational requirements and at least one year of experience in the field. Information on intended occupations is available for immigrants admitted to Canada since 1980. Reliable information is not available on the intended occupation of immigrants admitted under other admission categories (secondary applicants under the economic immigrant categories, sponsored by family and refugees).
Principal applicants who applied under the economic immigrant categories and were admitted since 1980 accounted for 52,220 adult immigrants (35.4%) in nursing or health care support occupations in 2016.
Definitions
Nursing and health care support occupations
When we refer to “nursing and health care support occupations,” we are referring to the following occupational groups taken from the 2016 National Occupational Classification (NOC):
- professional occupations in nursing
- nursing co-ordinators and supervisors (NOC code 3011)
- registered nurses and registered psychiatric nurses (NOC code 3012)
- licensed practical nurses (NOC code 3233)
- nurse aides, orderlies and patient service associates (NOC code 3413).
In most analyses, all professional occupations in nursing are grouped together because of the limited number of individuals classified in category 3011.
A person’s occupation corresponds to the main job held during the census reference week (in May 2016) or, if they did not work during that week, the longest job held since January 1, 2015. For data from the 1996 and 2006 censuses, the reference periods are similar (i.e., for the 1996 Census, the census reference week was in May 1996 and the period for longest job held was since January 1, 1995).
Adult immigrants
The term “adult immigrants” refers to people admitted to Canada as permanent residents at age 18 or older. “Non-immigrants and immigrants who arrived in Canada before the age of 18” refers to individuals who are not immigrants, who are temporary residents or who are immigrants who arrived in Canada before the age of 18.
Immigration admission category and applicant type
The admission category refers to the immigration program or group of programs under which immigration authorities first granted an immigrant the right to permanently live in Canada.
For the most part, this article uses the aggregate version of admission categories, which recognizes four main categories: economic immigrants, immigrants sponsored by family, refugees and other immigrants.Note For immigrants admitted under the economic immigrant categories, a distinction is made between those designated as the principal applicant on the application for permanent residence and those designated as secondary applicants (spouses or dependants).
The “caregivers” category refers to immigrants who were granted permanent resident status after providing home child care or care for people with care needs, such as the elderly, people with disabilities or people with a chronic disease, in Canada for a determinate period of time. Most immigrants in this category must have worked as a live-in employee in a private residence in Canada during their qualifying period of temporary work. Immigrants admitted under the Live-in Caregiver Program (which replaced the Foreign Domestic Program in 1992) are included in the caregiver applicant group. This group is part of the economic categories.
Overqualification of graduates of nursing programs
Graduates of some nursing and health care support programs are considered overqualified when they work in an occupation that requires a level of education lower than what they have. The study looks at two main categories of programs in the Classification of Instructional Programs (CIP):
- The licensed practical/vocational nurse instructional class (LPN, LVN, Cert., Dipl., AAS) (CIP code 51.3901), which refers to college-level educational programs that prepare graduates to assist in providing nursing care.
- Graduates of these programs are overqualified when they work in occupations that typically require no more than a high school education or job-specific or on-the-job training (National Occupational Classification skill levels C and D).
- The registered nursing, nursing administration, nursing research and clinical nursing instructional class (CIP code 51.38), which refers to college- and university-level educational programs that prepare graduates for professional occupations in nursing.
- Graduates with a bachelor’s degree or higher in these programs are overqualified for occupations that do not normally require a university degree (National Occupational Classification skill levels B, C and D).
- Graduates with a certificate or diploma below the bachelor level are overqualified for occupations that require no more than a high school education or job-specific or on-the-job training (National Occupational Classification skill levels C and D) or when working as a licensed practical nurse.
Multivariate analyses
In Table 5, binomial logistic regression models are used to account for the effect of age and province of residence on the probability of overqualification for those who studied in a given field and to calculate adjusted rates.
End of text box 2
Start of text box 3
Distribution of workers in nursing and health care support occupations, by occupation and region or country of birth, 2015/2016
| Region of birth/country of birth (selected cases) | Professional occupations in nursing | Licensed practical nurses | Nurse aides, orderlies and patient service associates |
|---|---|---|---|
| percentage | |||
| All workers | 48 | 11 | 40 |
| All adult immigrant workers | 35 | 11 | 55 |
| All other workersTable 6 Note 1 | 52 | 11 | 36 |
| United States | 62 | 8 | 31 |
| Central America | 15 | 9 | 76 |
| Caribbean and Bermuda | 26 | 11 | 63 |
| Haiti | 20 | 14 | 66 |
| Jamaica | 31 | 9 | 60 |
| South America | 28 | 10 | 62 |
| Guyana | 26 | 4 | 70 |
| Western Europe | 59 | 6 | 34 |
| Eastern Europe | 49 | 12 | 39 |
| Poland | 41 | 7 | 52 |
| Romania | 56 | 18 | 26 |
| Northern Europe | 63 | 6 | 31 |
| United Kingdom | 63 | 5 | 31 |
| Southern Europe | 33 | 8 | 59 |
| Western Africa | 35 | 8 | 57 |
| Nigeria | 40 | 6 | 54 |
| Ghana | 38 | 8 | 54 |
| Eastern Africa | 28 | 8 | 64 |
| Ethiopia | 18 | 8 | 74 |
| Northern Africa | 37 | 22 | 41 |
| Morocco | 30 | 25 | 45 |
| Central Africa | 26 | 11 | 63 |
| Democratic Republic of the Congo | 18 | 12 | 70 |
| Cameroon | 36 | 10 | 54 |
| Southern Africa | 62 | 4 | 34 |
| West Central Asia and the Middle East | 53 | 10 | 37 |
| Eastern Asia | 47 | 11 | 42 |
| China | 43 | 14 | 44 |
| Southeast Asia | 28 | 11 | 61 |
| Philippines | 28 | 11 | 61 |
| Southern Asia | 39 | 13 | 48 |
| India | 41 | 14 | 45 |
| Oceania | 42 | 10 | 48 |
End of text box 3
Start of text box 4
Occupation held by adult immigrants, by field and location of study, 2015/2016
| Major field of study | Occupation held | ||||||
|---|---|---|---|---|---|---|---|
| Professional occupations in nursing | Licensed practical nurses | Nurse aides, orderlies and patient service associates | Other health occupations | Non-health occupationsTable 7 Note 1 | |||
| Skill level A | Skill level B | Skill levels C and D | |||||
| percentage | |||||||
| Adult immigrants – Studies outside Canada | |||||||
| Caregivers, care attendants, patient attendants | 3 | 1 | 30 | 3 | 4 | 11 | 48 |
| Nursing assistants or aides and patient care assistants or aides | 6 | 4 | 16 | 2 | 5 | 16 | 50 |
| Licensed practical nurses | 14 | 16 | 13 | 2 | 3 | 11 | 41 |
| Registered nurses, nursing administration, nursing research and clinical nursing – Diploma below bachelor level | 35 | 5 | 12 | 3 | 7 | 11 | 28 |
| Registered nurses, nursing administration, nursing research and clinical nursing – Bachelor’s degree or higher | 37 | 7 | 17 | 3 | 5 | 7 | 24 |
| Adult immigrants – Studies in Canada | |||||||
| Caregivers, care attendants, patient attendants | 2 | 2 | 57 | 2 | 2 | 6 | 30 |
| Nursing assistants or aides and patient care assistants or aides | 9 | 17 | 41 | 1 | 3 | 6 | 22 |
| Licensed practical nurses | 18 | 52 | 11 | 2 | 2 | 4 | 11 |
| Registered nurses, nursing administration, nursing research and clinical nursing – Diploma below bachelor level | 60 | 14 | 10 | 1 | 3 | 4 | 8 |
| Registered nurses, nursing administration, nursing research and clinical nursing – Bachelor’s degree or higher | 78 | 3 | 3 | 3 | 7 | 2 | 4 |
| Non-immigrants and immigrants who arrived in Canada before the age of 18 | |||||||
| Caregivers, care attendants, patient attendants | 1 | 1 | 48 | 3 | 4 | 10 | 32 |
| Nursing assistants or aides and patient care assistants or aides | 11 | 13 | 22 | 2 | 7 | 12 | 32 |
| Licensed practical nurses | 14 | 49 | 8 | 2 | 5 | 7 | 15 |
| Registered nurses, nursing administration, nursing research and clinical nursing – Diploma below bachelor level | 65 | 6 | 3 | 2 | 7 | 7 | 10 |
| Registered nurses, nursing administration, nursing research and clinical nursing – Bachelor’s degree or higher | 76 | 1 | 2 | 3 | 10 | 3 | 5 |
End of text box 4
link